Appointments and scheduling: a programme of work for an open platform in NHS Wales
I propose a programme of work to demonstrate a new collaborative approach to technology across health and care in Wales, that recognises the fundamental, foundational requirement to understand a patient’s clinical encounters across disparate health and care services to create a “seamless” service via distributed modern technology.
While this is principally focused at health and care services in Wales, the design patterns have broad applicability, I hope.
One of the important principles is to sketch out a piece of work that helps us learn, rather than planning as if we have the answers. This is in line with our broad design principles.
Background
This is a programme of work that cuts across multiple workstreams of the Informed Health and Care strategy. These workstreams are:
- “Information for you”
- “Supporting professionals”
- “Improvement and innovation”
- “A planned future”
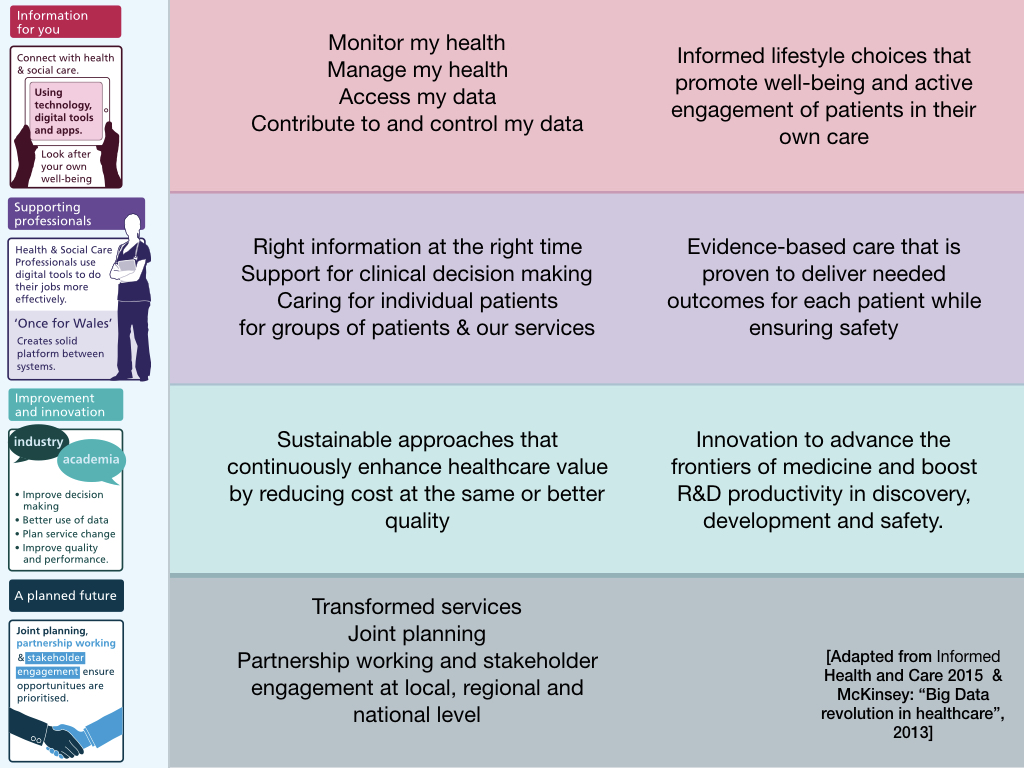
This isn’t a bad way of thinking about the challenges we face; for example, it provides some structure on which we can think about user needs. This is from my talk in 2017 at the inaugural Digital Health and Care Conference in Wales:
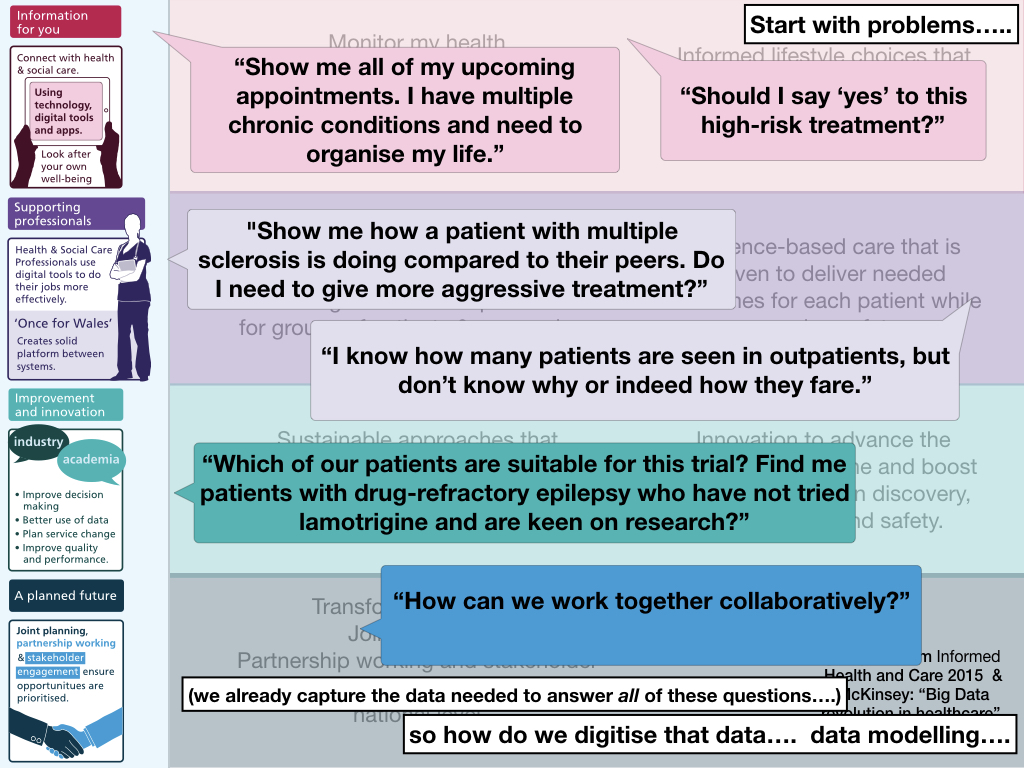
However, these workstreams aren’t the right way to structure the architecture, governance or programmes of work, because it is self-evident that there are important common software or data components that underpin delivery of the goals from more than one work-stream. It’s helpful to assess user needs and delivery via the prisms of these workstreams, but there’s something wrong in technological programmes of work all being under the responsibility of one of them.
A single seamless “system”
Our patients, their families and carers want our health services in Wales to work as a single seamless system, and the professionals that look after them, want to collaborate and work together to deliver that seamless care. This ‘single system’ approach aligns with the outcomes in “A Healthier Wales.”
At the moment, patients and families experience a patchwork of services that do not appear seamless at all. Some general practices permit booking of appointments electronically, but for many with multiple long-term health conditions, managing their appointments across the different health and care organisations is a difficult job.
Likewise, users of Welsh Clinical Portal see what appears to be a single application, but in fact see different data depending on where they are sitting. We see only that health board’s appointments in a specific version of WCP. This demonstrates a fundamental error in the design of currently deployed national applications. For example, last year I sat in my clinic in Cwm Taf and a patient was recorded as deceased while the same patient was recorded alive in Cardiff. We have single applications but multiple patient records. We must strive for a single patient record but we will always need to have multiple applications, customised for context (e.g. critical care, emergency units, primary care, analytics) and user (e.g. patient, professional).
Similarly, work on our “Single Cancer Pathway” highlights how important it is to understand the pathway of patients from diagnosis to treatment, and manage this seamlessly across organisational boundaries. We cannot interpret our performance and our outcomes without understanding what has happened to our patients. For too long we have separated data used by clinicians from that by managers and administrators, and none of it has been available to our patients.
Proposal
We need to create a core foundational national service to provide ‘appointments and scheduling’ services. Such a service needs to be a first-class “product” provided by the national ‘open’ platform.
Initially read-only, a view across multiple disparate systems including multiple PAS (patient administrative system), radiology and other systems including community care, providing a sane, standards-based API for use by multiple user-facing applications. It would be a unique and low-risk opportunity to build an architectural building block (ABB) that hides underlying complexity in favour of normalising and sanitising data from multiple sources to provide a seamless “single” record.
This development would need:
- a collaborative approach - we work across organisations in Wales
- a staged, incremental approach - it could start by providing only PAS data initially with additional integrations added piecemeal, not needing changes to applications using the API.
- to design for future change - including the ability to schedule appointments when the underlying services permit
Such an ABB would be used by multiple applications across multiple workstreams:
Workstream 1 - this component would be an important enabler to allow patients to see their appointments across primary, community and secondary care, including radiology.
We could provide a rudimentary patient portal, but also make those same data available via PKB and DrDoctor, and even via a demonstrator mobile application for NHS Wales, similar to that created by NHS Digital (The “NHS App”). If booking functionality is not provided by an underlying system (for example radiology), we could fake this functionality by providing a concierge service in which humans deal with requests and cancellations made via the service. This supports the identified “challenge project” within the recent architecture review of systems in NHS Wales.
Workstream 2 - allowing professionals to have a view of current, future and past appointments across our health and care organisations in Wales, no matter the site, or indeed which application, one is currently using.
This work would teach us a lot about APIs and application lifecycle management, logging, and access control, and would fit with need to modularise WCP as outlined in the architecture review, making it less tightly integrated - making it loosely-coupled - with the local PAS and instead providing a true national view of a single patient record. It also fits with the strategic theme, because booking staff could be alerted to clashes in booking; patients receiving appointments from different NHS and care organisations for the same date and time are not experiencing a seamless service.
A service does not feel seamless if you receive an appointment in one department or organisation that clashes with another.
Workstream 3 - we could feed scheduling information into a data warehouse and real-time analytics pipeline in order to understand our health and care demands across organisational boundaries in Wales, providing valuable learning to aid our “national data repository” work in an iterative, incremental way. This would teach us how to start to become data-driven, and use novel computationally intensive techniques to analyse streaming data in real-time.
Workstream 4 - this work, and particularly our use of open technical standards to drive interoperability, will teach us how we can deliver valuable software quickly and require collaboration across multiple teams. It will teach us whether we can do this work collaboratively in the ways I have outlined in this blog.
Alternative approaches?
Some people might suggest that the best way of delivering the outcomes I have outlined here would be to ensure a single “patient administrative system” for Wales, but such an approach would not solve breaking down the artificial silos we have built between primary and secondary care, or the hospital outpatients and, for example, radiology. Do we really want to force CAV to switch PAS? What a waste. Simply expose the right data, in the right format, for national use. In general, an organisation’s PAS supports local administrative workflows and anyone suggesting a rip and replacement approach to such a system should be questioned carefully.
Instead, we should look at how we can use software design patterns such as vendor neutral archives or a facade pattern to provide a seamless view across multiple disparate services and organisations, without impacting operational services.
The goal must be to have cohesive high-level strategic alignment of multiple, seemingly independent, products. For example, in this approach, work to identify patients who are likely to not attend for their appointments can be developed, tested and subsequently scaled out with ongoing evaluation and continuous improvement, without needing changes within other systems and across a complex, heterogeneous enterprise. That’s the power of adopting robust open technical standards and strategic planning.
Synergies
There are synergies with the following other programmes:
- Value-based healthcare / patient reported outcomes - appointments/scheduling form the foundation on which interventions and outcomes depend, and appointment data and scheduling functions would support patient-facing applications.
- Modular WCP - to show a coherent national view (“single patient record”) in patient portals, including WCP but also in ABHB’s CWS.
- NDR - national data resource - as part of workstream 3 - appointments and scheduling are a clearly defined domain which will provide valuable learning and permit an iterative, agile approach to development with early delivery of benefits.
- Phased planning with metered funding
Working on appointments and scheduling is one of the foundational building blocks of what would be a Welsh open platform (see https://wardle.org/strategy/2018/10/02/open-platform-wales.html)
It is a logical extension to the challenge projects identified in the architecture review - and identifies common core foundational challenges that underpin those projects - e.g. a modular WCP would need to view appointments from a single patient record, and not be tied to health board systems, e.g. a patient portal or mobile app would need a unified “one system” view across our health and care organisations but we’d want the same data to drive solutions such as PKB and our analytics as well.
Challenges and their mitigation
There are some obvious challenges, and I don’t have the answers yet. We need to fixed on creating teams that can solve these. We know from the most productive technology teams that the best way to deliver valuable software at pace is to work in an agile, iterative way.
There are some risks and some clear challenges that we will need to solve:
- Can Wales work together like this?
- Can we get access to systems which we cannot control?
- What’s the Myrddin (WelshPAS) database schema? Is it stable? Is it the same in different instances and configuration? Is there a standards-based API? What “standards” are used for encoding the information recorded, and are they harmonised between instances?
- What about Cardiff and Vale, who use a different PAS?
- Same question for RADIS, a ‘national’ radiology information system that is different in each organisation?
- Same question for GP systems? - we can’t have only a webview but we need the data itself. Are re-procurements sufficiently scoped to include what we would need to deliver our objectives?
- What community systems should we know about?
- What’s the minimum number of “systems” that we’d need to take data from, by stream replication or live API, to prove something useful?
- What would it take for health boards to use the toolbox of data and APIs that will be developed by this programme?
- What degree of churn is there in scheduling - do staff make changes repeatedly before the schedules are finalised and appointment letters sent out? How does this translate into a safe view for patients? Would you issue updates/notifications every 1, 2, 3, 6,8, or 24 hours?
- How do we solve the citizen identity/login issue? What work is there already in WG? What about gov.uk Verify? What does this look like, feel like for patients? Is it safe? Secure? High-risk/impact if we get this wrong?
- What’s the delegation model? Carers, parents, power of attorney? Has anyone solved this?
- Or can we fake it before we make it? Do we have to have patients login straightaway to a portal? What about making data available in PKB as part of that programme, and for anyone else, or everyone, nationalise the appointments/scheduling process so that letters are printed and sent out centrally? Are there economies of scale there? And doesn’t that mean we can get systems/processes right internally, and then safely switch over to electronic communications for those that opt-in? As a bonus, letters could go out to include the actual appointment letter, but also a wider NHS view - ie here are your other forthcoming appointments as well as this current appointment. Wouldn’t that make health and care much more seamless in feel? The idea is that on-the-ground, the teams doing scheduling wouldn’t have to necessarily know whether their patients are getting letters posted or sent electronically or by calendar invite!
- Do we have a canonical source of “communication preferences” for citizens? I’ve seen this referenced in different PAS, but is it joined up? What are the scenarios? eg I’m a student and I want my appointments/schedule via mobile/email and also a letter to my parents. Or not. Or most of the time, except for this clinic. How does this work for different clinical environments? What about the GU clinic?
- Can we use the same approach to help patients who receive cross-border care - for example, North Wales and tertiary centres in Liverpool, the Birmingham liver service etc. What would we need to do to our approach to include data from other nations of the UK? Can we take advantage of the push towards open standards, the inception of NHSX and our collaborations with organisations such as HL7, INTEROpen etc.?
- What are the technical standards needed here, and how do we align across the border?
- If we’re combining appointment and scheduling data from disparate systems, is our demographic matching infrastructure (EMPI) up to the challenge? My testing suggests very slow response times against the test instance (>2s) so how could that be mitigated? Is a cache needed? What ‘fitness functions’ should be used to define the operational standards we expect from these services?
- How can we limit our interactions with the “demographics” programme of work by adopting appropriate technical standards (API definitions, security, authentication, authorisation, scalability, responsiveness, quality of service indicators), so that we can work independently but rely on a single view of demographic information?
Next steps
This is not a project but instead we are building and delivering services and products. We can be clear about our overall direction; we are opening up our architecture, building a data-driven learning health and care system that appears, to patients and professionals, as increasing seamless. However, we will find hurdles and difficulties not yet imagined, and so we must look to defer decisions until the last possible moment so that we minimise risk. We do not minimise risk by planning and developing long lists of requirements by stakeholders, but instead delivering software again and again and getting fast feedback.
The next steps must be focused on building capacity and capability - and identifying the obvious challenges - and then building teams, made up of different specialisms, working collaboratively, empowered and trusted, to deliver solutions to those challenges and teach the wider programme what worked and what didn’t.
We don’t have all of the answers. Let’s create work that teaches us.
Mark
Addendum
What press releases might come about from this programme?
Thinking about press release content is an interesting way to ensure we are aligning our technology programmes and the products/services that will be built to our wider health and care strategic goals. We can write a short press release, either for a programme or a specific service. This is something that organisations such as Amazon use in order to work out whether something is valuable.
We challenge ourselves: are we doing something valuable here?
I’ve never tried this before, and I’m not a public relations expert, so these are simply a way of thinking about a problem, not an actual press release!
But, outcomes in digital / technology are health and care outcomes. We need to stop thinking of digital (and IT) as a separate department or organisation, but instead focus on benefits for patients, carers and professionals. Digital technology is the enabler.
So here are two example press releases to illustrate the importance of this work.
1. Seamless health and care in NHS Wales
As part of its “A Healthier Wales” programme, NHS Wales has announced a new patient and carer-focused approach to healthcare data. Stating the importance of a “single patient record” and the need for a “single seamless system” across all organisations providing health and care services, patient data will be made available via portals, mobile applications and third-parties.
“We have been experimenting with products like ‘XXXX’ and ‘YYYY’ to provide ways for patients to see and contribute to their record,” says Dr xxxx, Chief Digital Officer for NHS Wales, “but these experiments have been piecemeal. Our approach is to focus on bringing together information from across Wales and making that available for patients and professionals by adopting open standards to support interoperability across Wales. Initially, patients and their representatives will be able to manage their appointments via a variety of channels, such as our new patient portal, an NHS Wales application and via third party providers such as XXX and YYYY but we expect to rollout additional functionality incrementally over time.”
Speaking at the XXX event, Dr XXXX talked about the collaboration with partners across the UK so that patients receiving care from NHS services in other nations of the UK will experience a more joined-up and seamless service, irrespective of where they attend.
2. A new approach to managing outpatients using AI.
NHS Wales has announced a new national approach to scheduling and managing outpatients appointments. In collaboration with xxxx University, advanced mathematical algorithms and machine learning will identify patients most at need. “For example, additional support will be provided to patients predicted to be at higher risk of missing appointments”, says Dr XXXX, “our Healthier Wales programme is focused on a person-centred approach in which care, irrespective of where and how it is provided, is seamless and joined-up. We can use data to identify those most in need of help, particularly those with long-term health conditions.”